IASR 43(2), 2022【THE TOPIC OF THIS MONTH】 Shigellosis 2010-2021
PDF download(PDF:513KB)
The topic of This Month Vol.43 No.2(No. 504)![]()
Shigellosis 2010-2021
(IASR Vol. 43 p25-27:February 2022)
Shigellosis is caused by the bacterium Shigella spp.. The main symptoms are fever, watery diarrhea, abdominal pain, purulent bloody stools, and tenesmus. It is estimated that 270 million people were infected and approximately 210,000 people died due to shigellosis worldwide in 2016, mostly children with poor nutrition (GBD 2016 Diarrhoeal Disease Collaborators, 2018). The genus Shigella consists of four species: Shigella dysenteriae, S. flexneri, S. boydii, and S. sonnei. In particular, some S. dysenteriae serotype 1 (Sd1) strains are highly pathogenic because they can produce shiga toxin, Stx1, which is also produced by enterohemorrhagic Escherichia coli. Shigella is reported to be experimentally infectious at low levels, ranging from tens to hundreds of organisms (Morris, 1986).
Shigellosis is classified as a Category III Infectious Disease under the Infectious Diseases Control Law. When a physician diagnoses shigellosis, they must immediately notify the public health center (PHC) (https://www.mhlw.go.jp/bunya/kenkou/kekkaku-kansenshou11/01-03-02.html). The PHC reports the information to the National Epidemiological Surveillance of Infectious Diseases (NESID) system. Shigella is also defined as a causative agent of food poisoning under the Food Sanitation Law. If the director of the PHC recognizes the case as food poisoning, the local government conducts an investigation of food poisoning and reports it to the Ministry of Health, Labour and Welfare (MHLW) based on the Food Sanitation Law [Food Sanitation Law: https://elaws.e-gov.go.jp/document?lawid=322AC0000000233, Enforcement of the Food Sanitation Law (Enforcement, etc. of the Ministerial Ordinance for Partial Amendments to Regulations of the Food Sanitation Law: https://www.mhlw.go.jp/www1/topics/syokueihou/tp1228-1_13.html)]. Prefectural and municipal public health institutes (PHI) perform isolation, identification, and serotyping of the organisms. The Department of Bacteriology I of the National Institute of Infectious Diseases (NIID) confirms the isolates sent by the PHI and performs molecular epidemiological analysis using multilocus variable-number tandem-repeat analysis (MLVA) and pulsed-field gel electrophoresis (PFGE). The results of these analyses are fed back to the PHIs, and, as necessary, are provided to MHLW and relevant local governments.
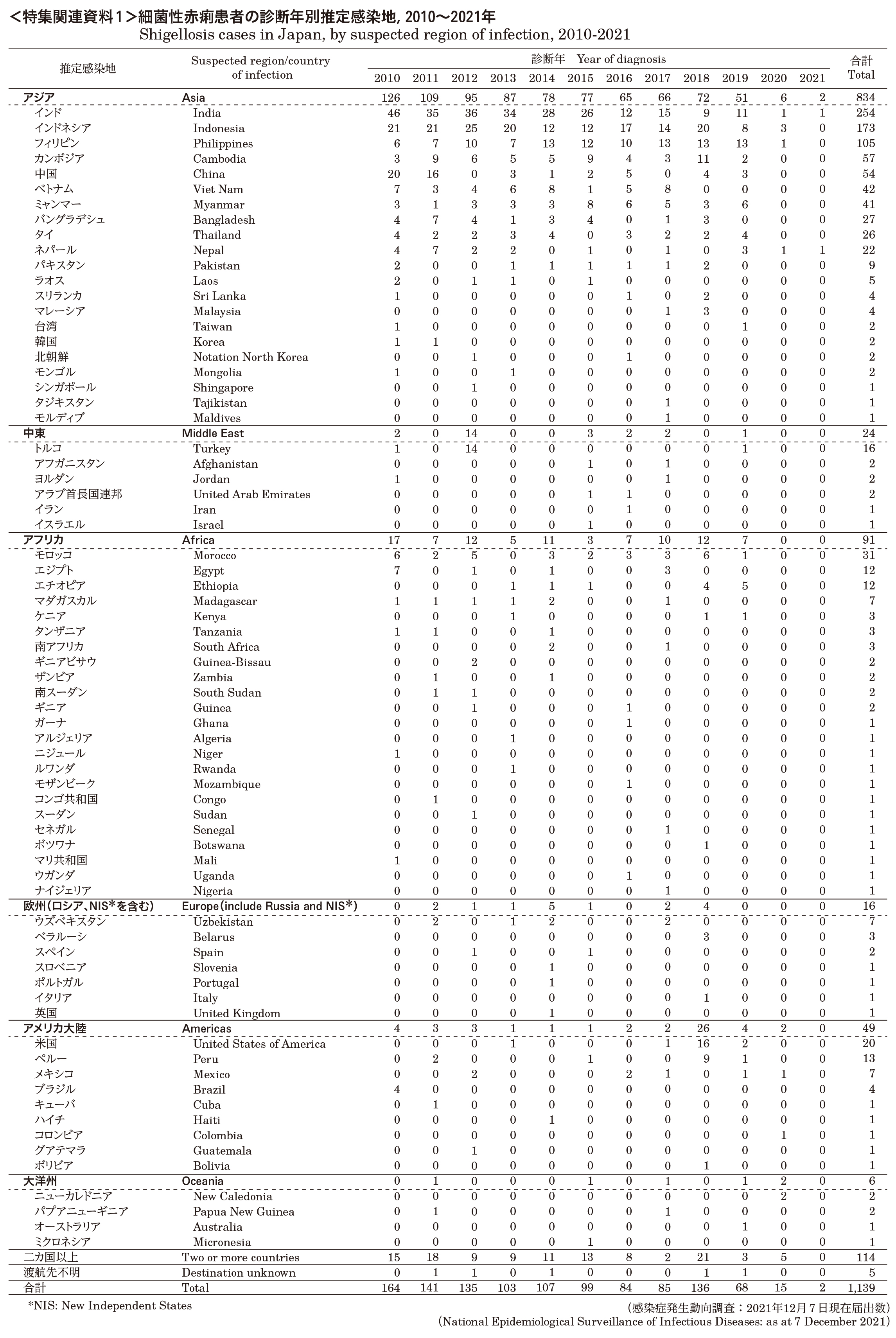
National Epidemiological Surveillance of Infectious Diseases (NESID): According to the NESID system, the numbers of notified cases of shigellosis including symptomatic cases and asymptomatic cases were as follows: 235 cases in 2010, 299 in 2011, 215 in 2012, 143 in 2013, 159 in 2014, 155 in 2015, 121 in 2016, 141 in 2017, 268 in 2018, 140 in 2019, 87 in 2020, and 7 in 2021, for a total of 1,970 cases, as at 7 December, 2021 (Table 1). The average number of notifications per year from 2010 to 2021 was 164. As for the suspected place of infection, imported cases made up 58% of the cases. Asia accounted for 75% of the imported cases, with India, Indonesia, and the Philippines being the top 3 (see p.27).
The number of notifications by month of diagnosis shows that the number of imported cases tends to be higher in the periods when people are more likely to take long vacations (e.g., summer), although cases were observed throughout the year. There have been very few cases since April 2020, however (Fig. 1a, see p.28 of this issue). Domestic case counts have fluctuated from year to year, and peaks corresponding to outbreaks and food poisoning occurrences have been observed, although they have generally remained at low levels (Fig. 1b).
Regarding the age distribution of the notified cases from 2010 to 2021, imported cases showed a peak in the younger group aged 20 to 34 years (Fig. 2a). On the other hand, among domestic cases, there were many in those aged less than 10 years, followed by those aged 30 to 44 years (Fig. 2b). In terms of gender distribution, 973 cases were male and 997 were female. Imported cases were most numerous in the 20-34-year age group, with females outnumbering males. Among domestic cases, cases were most numerous in the 30 -44-year age group, with a male predominance.
Outbreaks: According to the food poisoning statistics of MHLW, the number of shigella food poisoning events reported were 1 in 2010, 7 in 2011, and 2 in 2018, totaling 10 outbreaks, affecting 169 persons (see p.28 of this issue). The most common facilities attributed as the source were restaurants and caterers (see p.30 of this issue). There have also been some clusters of cases and outbreaks reported in kindergartens and nurseries (see p.31 of this issue, IASR 32: 171-172, 2011, IASR 33: 245-247, 2012, IASR 38: 103-104, 2017). Molecular epidemiological analyses done at the Department of Bacteriology I of NIID have identified clusters of matching or similar strains, including in some of these outbreaks (see p.32 of this issue).
Shigella isolated by PHIs: PHIs reported 739 isolates of Shigella spp. during 2010 and 2021. The contribution of S. sonnei remained high, accounting for 541 (73%), followed by S. flexneri with 171 (23%). The numbers of S. dysenteriae and S. boydii were 5 (0.7%) and 19 (2.6%), respectively (Table. 2).
Treatment and antimicrobial resistance (AMR): “The Japanese Society of Infectious Diseases (JAID)/ Japan Society of Chemotherapy (JSC) Guide to the Treatment of Infectious Diseases 2019” published by JAID/JSC recommends 500 mg levofloxacin for 5 days, 300 mg azithromycin for 3 days, and 2 g fosfomycin for 5 days. Compared to the previous issue in 2009 (IASR 30: 311-313, 2009), the dose of levofloxacin was increased (from 300 to 500 mg) and azithromycin was added. This is due to an increase in AMR. The report “Antibiotic Resistance Threats in the United States, 2019” by the Centers for Disease Control and Prevention (CDC) lists antimicrobial-resistant Shigella spp. as a serious threat. Most strains of Shigella isolated in Japan are indeed resistant to drugs such as sulfamethoxazole-trimethoprim (ST) (see p.33 of this issue). Detections of ciprofloxacin-resistant and azithromycin-low-susceptible strains have been reported overseas (see p.34 of this issue), and such resistant strains may also become a threat to our country in the future.
Prevention and measures to be implemented: In recent years, most cases of shigellosis in Japan have been caused by overseas travel or secondary infection from such persons infected overseas. In the past, outbreaks of food poisoning associated with imported seafood have occurred, and the monitoring system for imported foods has been strengthened (IASR 24: 1-2, 2003, IASR 30: 311-313, 2009). As Shigella infection is established with a small number of bacteria, shigellosis can spread easily and poses a public health concern. To prevent secondary infections, it is important to identify patients and carriers as early as possible, treat them, and ensure that they are not shedding bacteria. The low infectious dose often makes it diff icult to identify the food source causing the food poisoning, or the cause remains unknown even when outbreaks occur in Japan. A case has been reported in which a person who had been infected abroad engaged in food-related work, despite having symptoms after returning to Japan (IASR 28: 326-327, 2007). Therefore, it is necessary to disseminate knowledge about imported infectious diseases and to raise awareness regarding the importance of health counseling at quarantine stations and PHCs if there is any suspicion of infection upon returning to Japan.
Shigellosis is easily transmitted from human to human by the fecal-oral route. Outbreaks among men who have sex with men (MSM) have also been reported overseas (see p.34 of this issue, IASR 33: 17, 2012, IASR 33: 170-171, 2012). In environments with many compromised hosts and weak infection control, such as nursery schools, daycare centers and facilities for the disabled, it is important to carry out tests and identify infected individuals even in cases of mild illness because there is a high likelihood of infection spreading from infected persons with mild symptoms or asymptomatic carriers.
Compared to the number of case reports of shigellosis from physicians to NESID, the number of reports of Shigella registered in NESID’s pathogen reporting system (laboratory-based surveillance; Infectious Agents Surveillance System) by PHIs and PHCs is approximately one-third. According to the enforcement regulations of the Infectious Diseases Control Law, PHCs are allowed to actively request medical facilities and private laboratories to submit isolates of Shigella when there is a notification of a case-patient. For the investigation of infectious diseases and food poisoning events, it is extremely important to analyze the isolates using molecular epidemiology and to assess for antimicrobial resistance; doing so allows for the provision of appropriate medical care to patients, recognition of outbreaks, detection of widespread or sporadic occurrences, determination of the cause, and prevention of future outbreaks. Based on the notice (https://www.mhlw.go.jp/file/06-Seisakujouhou-10900000-Kenkoukyoku/2_7_05.pdf), PHCs and PHIs are encouraged to collect isolates and send them to NIID for analysis.

{kind=link}